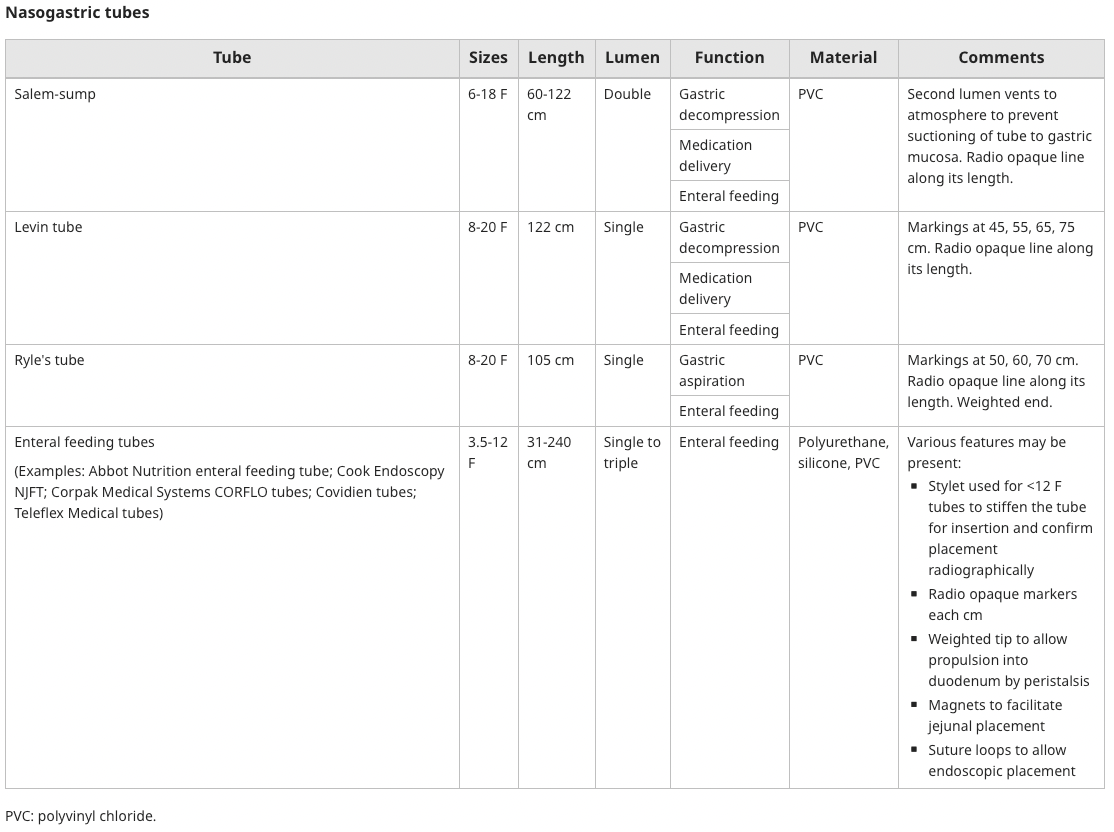
Nasogastric Tubes
These would be heinous uncomfortable.

Steps
1) Define indication for nasogastric tubes (NGTs).
There are two broad categories of indications for NGTs:
- Take stuff out (aspiration/lavage).
- Treatment of ileus or bowel obstruction → gastrointestinal decompression improves patient comfort, minimizes or prevents recurrent vomiting and allows for monitoring of progression
- Lavage may be needed to remove blood or clots to facilitate endoscopy, rarely in poisoning
- Put stuff in (feeding/rehydration/medication administration).
- Enteral nutrition
- Administration of medications or oral contrast
2) Ensure there are no contraindications.
- Oesophageal stricture → high risk of perforation
- Facial or basal skull trauma & fracture → potential for intracranial misplacement
- Oesophageal varices → high-risk of life-threatening bleeding
- Bleeding diathesis → minimal trauma may lead to severe bleeding
3) Collect equipment.
- Towel to lay down on the patient's chest to mop up any secretions or vomitus that comes up.
- Non-sterile gloves.
- Anaesthetic spray (with long attachment to send to back of nasopharynx and oropharynx).
- Lubricant gel.
- Nasogastric tube. Approximate size is ~60cm for adults, but measure from nasal alar (or nares/nostrils) to tragus and down to xiphisternum, then add 5-10cm.
- Cup with water (+ straw).
- Special bag for attachment to end of NGT for emptying of contents.
- 50mL syringe for aspiration.
- Tape for tying NGT to nose.
- Extra tape + scissors for taping rest of tubing down.
- Extra hands (not always needed)
4) Consent the patient.
For example:
Hi, my name is XX and I'm one of the doctors looking after you. I know that you've been suffering from some vomiting and so to help reduce this, we want to put a nasogastric tube into your stomach. Is this ever something you've had done before? It's a relatively straightforward procedure that will involve putting this tube down your nose, down your oesophagus or your eating tube and into your stomach. To make the process a little less uncomfortable, we'll be doing a couple of things: 1) We'll put some gel on the tube, 2) We'll spray the back of your throat and nose with an anaesthetic spray that will reduce any pain associated with getting it down at the start. As with any procedure, there are some risks to this. The main ones are: 1) Risk of trauma and bleeding to the nose, but we'll be careful to try and ensure that doesn't happen, 2) Incorrectly placing the tube into your lungs as opposed to your stomach, but we'll be mitigating that risk by getting you to swallow water as we push, which should help direct the tube into the stomach, as well as doing an x-ray afterwards to check that the tube is in the right place. Now, once the tube is in your tummy, we'll be able to suck away any of the stuff that's lying around in your stomach that's contributing to your vomiting. Does that sound ok with you? Are you happy for me to proceed? If at any time you feel too uncomfortable, just tap me on the shoulder and we'll stop and see if we can work around that.
4) Set up the environment.
- Patient should be lying upright in bed, as flat as possible. It’s ok for them to be flat even if they have heart failure because the flatter they are the straighter the urethra will be which makes your job easier and in 5 mins they won’t be too symptomatic.
- Stand on the side so that you have your dominant hand over the patient that you can use to thread the NGT into the patient's nose.
- Have the bed at the right height.
- Have a cart with your equipment on it behind/lateral to you (or place equipment on the patient's bed).
- Get patient to hold cup of water.
5) Spray the nasopharynx and oropharynx.
Ensure that you keep the spray nozzle flat (i.e. parallel to the ground). Wait a minute or two before proceeding.
6) Attach the bag to the end of the tube.
7) Lubricate the tube with gel.
8) Insert the tube until you feel resistance (this is the back of the nasopharynx).
Twist tube 180° to get past this and to try and prevent tube curling back into mouth.
9) Advise the patient to begin swallowing water.
Advance the tube with each swallow of water.
10) Continue pushing the tube until you reach the mark you measured before.
If the patient starts coughing, you may be in the trachea/bronchi. Pull back and re-try whilst patient is swallowing.
11) Aspirate to see if any gastric contents appear (or observe filling of bag).
12) Tape the NGT to the patient's nose.
13) Tape the rest of the tube down to the patient so it's not in the way.
14) Hang the bag.
15) Organise chest x-ray to ensure NGT is in correct position.
The correct position is that you can visualise the NGT passing midline through the thorax, past the carina, and ending under the left hemi-diaphragm in the general region of the stomach.

Resources
- Surgical Registrar
- UpToDate: Inpatient placement and management of nasogastric and nasoenteric tubes in adults
- GeekyMedics: Assessing Nasogastric (NG) Tube Placement