Hyperkalaemia
Be careful not to eat too many bananas.

High-Yield Tips
- Always check Therapeutic Guidelines or your local guidelines prior to actually dosing a patient (as this information may be out of date by the time you read it)
- If serum [K] > 6.5, it is quite concerning
- Management
- ECG
- IV calcium gluconate
- IV dextrose 50% + insulin (alternatively, salbutamol)
- Resonium
- IV sodium bicarbonate (if metabolic acidosis present)
- 0.9% sodium chloride for rehydration
Definition
Serum potassium concentration > 5.2 mmol/L.
Normal range: 3.5-5.2 mmol/L
Classification
- Mild: 5.2 < serum [potassium] ≤ 6.0
- Moderate: 6.0 < serum [potassium] ≤ 7.0
- Severe: serum [potassium] > 7.0
Aetiology
Is it pseudohyperkalaemia or true hyperkalaemia?
- Pseudohyperkalaemia: falsely elevated serum [potassium]. Causes include:
- Mechanical trauma during venepuncture → cell lysis → K release
- Clotting (in a patient with thrombocytosis) → K moves out of platelets
- Sample obtained from vein proximal to site of K infusion
- True hyperkalaemia causes:
- ↑ K release from cells
- Metabolic acidosis (other than lactic acidosis or ketoacidosis)
- Rare to see hyperkalaemia caused by respiratory acidosis too
- Insulin deficiency (+/- combined with hyperglycaemia and hyperosmolality)
- Mechanism: (normally insulin promotes K entry into cells) in an insulin-deficient state with hyperglycaemia and hyperosmolality
- → water moves by osmosis from within cells to ECF → raises intracelullar [K] → favourable gradient for passive movement of K to ECF
- → body in 'fasting state' + insulin not able to inhibit β-oxidation → ketosis → ketoacidosis → H/K co-transporter shifts protons intracellularly in exchange for K to minimise extracellular acid-base disturbances → hyperkalaemia
- Mechanism: (normally insulin promotes K entry into cells) in an insulin-deficient state with hyperglycaemia and hyperosmolality
- Other causes of ↓ insulin levels
- Somatostatin (or analogues e.g. octreotide)
- Fasting
- ↑ tissue catabolism
- Trauma
- Rhabdomyolysis
- Tumour lysis syndrome
- Severe hypothermia
- Other
- Overdose of digitalis or related digitalis glycosides
- Red cell transfusion
- Succinylcholine
- K absorption from GIT bleed
- Hyperkalaemic periodic paralysis
- Metabolic acidosis (other than lactic acidosis or ketoacidosis)
- ↓ urinary K excretion
- ↓ ALD secretion
- ↓ response to aldosterone (e.g. use of K-sparing diuretics aka aldosterone antagonists)
- ↓ distal sodium and water delivery 2° to hypovolaemia
- Acute and chronic kidney disease
- ↑ K release from cells
Clinical Manifestations
- Muscle weakness or paralysis
- Cardiac conduction abnormalities and arrhythmias
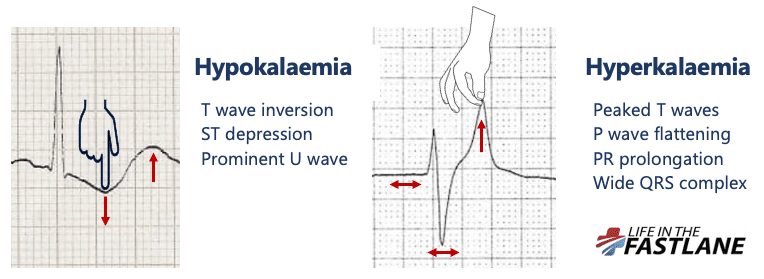
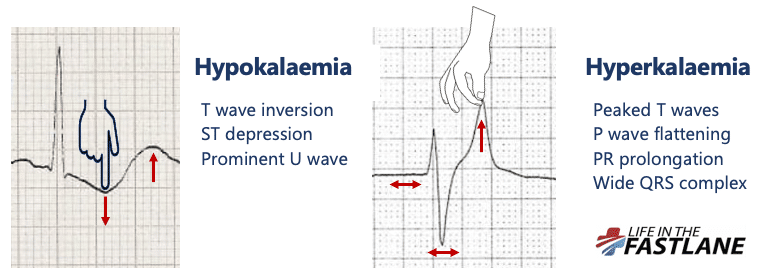
ECG Changes
Changes usually progress as serum [K] increases.
- 5.5-6.5 mmol/L: Tall peaked T waves
- 6.5-7.5 mmol/L: Loss of P waves, prolonged PR interval
- 7.0-8.0 mmol/L: Widening of QRS complex
- 8.0-10.0 mmol/L: Sine wave, ventricular arrhythmia, asystole
Management
Emergency Management
- Primary survey
- ECG (or telemetry preferred for continuous monitoring)
- IV calcium gluconate 10% 10mL IV over 2-3 mins into a large vein
- Note: effect of this infusion is short-lived and dose may need to be repeated in 30-60 mins whilst simultaneously undertaking measures to reduce potassium
- Purpose: stabilise cardiac membrane to prevent cardiac arrest
- Indication: cardiac arrhythmia or severe ECG changes of acute hyperkalaemia
- IV sodium bicarbonate 8.4% 50mL IV over 5-10 mins
- Purpose: correction of volume depletion (if present) + any underlying metabolic acidosis
- May be repeated in 60-120 mins
- Fluid replacement may need to be continued with sodium chloride 0.9%
- Glucose 50% 50mL IV over 5 mins + short-acting insulin (e.g. aspart 100 units/mL) 10 units IV bolus
- Note: MUST give dextrose before insulin as dextrose can compromise cannula and if insulin is given first and subsequent glucose not given → hypoglycaemia
- Glucose 50% may cause vascular irritation
- Alternatively to above regimen of Glucose 50%, can give glucose 10% 250mL over 15 mins
- Consider ongoing monitoring of BSL and need for further glucose + insulin
- Effective in renal failure
- Nebulised salbutamol e.g. 5mg neb q1-2h (max 10-20mg in 24h)
- Can be given as an alternative to glucose + insulin to temporarily shift K intracellularly
- 10 mg salbutamol may lower K by 0.5-1.0 mmol/L by 15-30 mins, with effect lasting ~ 2h
- Cessation of any exacerbating medications e.g. potassium-sparing diuretics
- Sodium polystyrene sulfonate 15g (suspended in 45-60mL of water) PO TDS or QID
- Purpose: to reduce GIT potassium absorption
- This treatment lowers the serum potassium concentration by 0.5 to 1 mmol/L over 1 to 6 hours.
- Note: as sodium polystyrene can ↑ Na, consider calcium polystyrene sulfonate (same dose) instead
- Situational treatment options:
- Dialysis
- Corticosteroid replacement (e.g. IV hydrocortisone) if aetiology is adrenal insufficiency and hypoaldosteronism + don't use insulin
Resources
- LITFL: Hyperkalaemia
- UpToDate: Causes and evaluation of hyperkalemia in adults
- UpToDate: Clinical manifestations of hyperkalaemia in adults
- Therapeutic Guidelines: Hyperkalaemia




{kind=link}